
These are The Topics:
Lackluster Results of Botox: When the Magic Fades Away
Unlocking the Reliability of Botox Effects: A Game-Changer in Aesthetics
Unveiling the Truth: Addressing Criticism Towards the Doctor’s Role in Botox Treatment
Understanding Botox Resistance and Its Impact on Treatment
Botox Isn’t Working for Me – What Are My Options?
FAQ: Understanding How Botox Works and When to Expect Results

Unlocking the Reliability of Botox Effects: A Game-Changer in Aesthetics
Promising Results: High Satisfaction Rates and Positive Feedback
The Good News First: The finding that Botox remains ineffective is rare. On the contrary, the therapy even shines with high satisfaction rates of 80-90%. Studies confirm this again and again. For instance, one study suggests that 9 out of 10 people treated with Botox are satisfied with the results and still feel significantly better four months after treatment. Only a few subjects reported negative experiences with Botox. Far more were convinced by the effect and would definitely recommend Botox.
Positive Effects Beyond Aesthetics: Botox and Improved Well-being
Another study proves that people who had their forehead treated with Botox were significantly happier afterward than the control group. This coincides with the well-documented suspicion that Botox can help with depression. Can these studies always be generalized and in every aspect? Maybe not. But the conclusion remains: Botox is usually very reliable.
Disappointing Results: Understanding Botox Treatment Failures
And yet, there are instances where Botox doesn’t show any effect. Or that the effect at least falls short of expectations. Patients are then rightly disappointed. Not least for financial reasons: costs of several hundred dollars are not met with a result that would be worth this effort.
Frustration and Hope: The Impact of Botox Treatment Failures
But often it’s about more than just money or a younger appearance: those who use Botox for certain ailments, such as spasms, dystonias, or migraine and bruxism, hope for a genuine increase in their well-being. Moreover, many patients have to overcome their fears of Botox first. The frustration is then all the greater when the therapy fails and the hoped-for effect does not occur. And unfortunately, in neurological therapy, Botox frequently does not work as hoped.
Managing Expectations: Botox Treatment for Chronic Migraines
One example: With the approval of Botox for chronic migraine, it was clear that the therapy would fail in a relatively high percentage of patients. However, you usually only know whether you are such a patient in retrospect. And with all that we know today about the exact mechanisms behind the Botox effect or don’t know, you can often only say: unfortunately, bad luck!
Realistic Expectations: The Role of the Doctor in Aesthetic Medicine
One of the central tasks of a doctor is to keep the expectations of his patients at a realistic level. And in aesthetic medicine, that is often enough of a challenge. Because one’s own appearance is judged emotionally and expectations of a cosmetic procedure are regularly exaggerated. Furthermore, aesthetic medicine is often accompanied by an overabundance of promises, with many individuals within the field seeking to capitalize on it.
Patience is Key: Understanding the Timing of Botox Effects
The question of when to expect an effect from Botox also contributes to false expectations. Unfortunately, many have become accustomed to having “everything immediately.” But that’s not the case with the effect of Botox. It only sets in after a few days. This has biochemical reasons, which I will go into in more detail at the end of the text.
Unveiling the Truth: Addressing Criticism Towards the Doctor’s Role in Botox Treatment
The Role of the Doctor in Treatment Failures
At this point in the text, it is evident that primary therapeutic failure of Botox typically falls on the responsibility of the doctor. If the expectations of the outcome were too high, the doctor should have tempered them to a realistic level. Additionally, if the indication was incorrect and Botox was not an appropriate treatment from the start, it simply amounts to misdiagnosis. In practice, the majority of cases where Botox shows no effect can very likely be categorized into one of these two scenarios.
The Importance of Proper Administration and Preparation
A third reason, for which the doctor is also accountable, lies in the improper preparation and application of the toxin. This includes errors in storage. While Botox is not an overly sensitive medication, it must be stored at a specific temperature in the refrigerator to maintain its full effect. Furthermore, Botox must be diluted with saline solution in precise proportions before being administered to the patient. However, in its diluted state, it should only be stored for a short period. Can errors be made in all these steps that could result in a loss of Botox’s effectiveness? Absolutely!
Bridging the Gap: Communication and Assessment of Results
Another aspect in which the doctor plays a crucial role is in assessing the treatment’s outcome. It is possible that the doctor and the patient may have differing opinions. Of course, if a frown line is still just as prominent despite Botox, there is no room for argument. However, it is not always so clear-cut. If the patient feels that the Botox had no effect, but the doctor sees success, there is clearly a disagreement. Studies have indeed shown that doctors and patients perceive the effects of Botox differently compared to a placebo. However, doctors were more accurate in their assessments than the treated patients.
The Importance of Communication and Documentation in Assessing Botox Treatment Results
In such situations, only a clarifying conversation can help. A conscientious doctor will have documented the initial condition verbally and with photos. Therefore, it should be possible to compare the outcome with the baseline and discuss the differences objectively. In my experience, this requires a personal conversation. This ensures comparability because with all the selfies that patients spontaneously send via email or messenger in such cases, it is immediately apparent that the lighting conditions during the capture render comparability impossible. As a doctor, one can only advocate for evaluating the post-treatment condition under the same conditions as the baseline. This includes similar lighting conditions in the doctor’s office. Only then can results be objectively discussed and disagreement prevented.
The Doctor’s Responsibility: Avoiding Misdiagnoses
Misdiagnoses and errors in application are the responsibility of the doctor. There is no need for debate on this matter. If Botox is injected for wrinkles that are not of mimetic origin, failure is inevitable. The muscular relaxation that the toxin is intended to produce may occur exactly as planned, but it will not contribute to improving the appearance of these particular wrinkles. Examples include sagging wrinkles or the nasolabial fold, which are not treatable with Botox. There are other techniques that can successfully mitigate them, but negative experiences are guaranteed with Botox.
Understanding Muscle Tone and Realistic Expectations
A similar, and probably quite common, issue lies in underestimating muscle tone and overestimating the effects of Botox. Muscle tone refers to the baseline tension present in a muscle even in a relaxed state. While Botox does induce relaxation, it may not be sufficient to completely eliminate wrinkles. Alternatively, the wrinkles may initially disappear, but the effects of Botox seem to vanish after only three months. An experienced doctor should not encounter such situations. While there may be cases that are difficult to evaluate and where the effects are not precisely predictable, it is then the doctor’s responsibility to warn the patient about the associated risks and manage their expectations accordingly.
Differentiating Patient Types: Insights from Dr. Mauricio de Maio
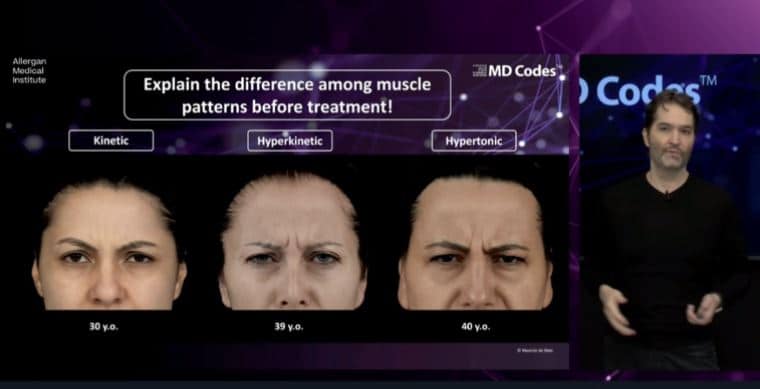
Brazilian plastic surgeon and Botox expert, Mauricio de Maio, distinguishes between three patient types: kinetic, hyperkinetic, and hypertonic.
For kinetic patients, the pattern of wrinkles corresponds to facial expressions, appearing only when they laugh or furrow their brows. With such patients, the expected Botox effects are likely to occur and can last a full 6 months.
In the case of hyperkinetic patients, their facial muscles are overactive, constantly in motion when they speak or even when they are attentive. According to de Maio, the initial effects of Botox should work well for them, too. However, the duration of the effects becomes questionable, typically lasting only 3–4 months.
Finally, hypertonic patients have muscles already tensed to such an extent that Botox cannot achieve complete relaxation. While the appearance of wrinkles may improve, they will never fully disappear. The effects of Botox in such patients are also significantly shortened, lasting approximately 3 months.
As seen in the following screenshot from an online training, de Maio strongly advocates informing patients about these variations before treatment. This enables them to form realistic expectations and avoids negative experiences with Botox due to unmet high expectations.
Identifying and Preventing Common Application Mistakes
Application errors occur when the Botox treatment is correctly indicated but not executed properly. Several cases can arise:
Insufficient Botox dosage
Injections not targeting the correct muscles
Incorrect injection technique
Quality deficiencies in the Botox syringe (e.g., due to improper storage)
Again, it can be observed that experienced Botox practitioners generally avoid such errors. As mentioned earlier regarding indications, there may be borderline cases where the muscular anatomy poses a risk of injecting the wrong muscle, resulting in the desired effect on wrinkles not being achieved. The doctor must address this issue beforehand and inform the patient about the associated risks.
Furthermore, injecting the wrong muscle can lead not only to the cosmetic effect being absent but also to undesired cosmetic consequences. Frequent examples include the dreaded “Spock eyebrows” or drooping corners of the mouth.
Leaving the patient unaware of these risks can result in not only the patient complaining about the lack of effectiveness but also being dismayed by unforeseen effects. Comprehensive patient education is essential to prevent unnecessary negative experiences with Botox, both in terms of effectiveness and unwanted outcomes.
Understanding Botox Resistance and Its Impact on Treatment
Overcoming Challenges: Exploring Botox Resistance
We have discussed the patient’s high expectations and the doctor’s treatment errors as potential causes for Botox treatment failures. However, now let’s explore a third possible cause for which the doctor is generally not at fault: Botox resistance. This occurs when the patient develops antibodies against Botox, resulting in an immune reaction that inhibits the effectiveness of Botox.
Dispelling Common Misconceptions about Botox Resistance
Botox resistance happens much less frequently than commonly believed and is almost non-existent in cosmetic Botox therapy. The few cases of Botox resistance primarily affect patients undergoing treatment for spasms or dystonias, which require very high doses of the medication. For example, studies with dystonia patients have shown Botox resistance in 3-10% of cases after repeated treatments.
How does Botox resistance occur?
Antibodies Binding to Active Molecules
Botox contains biologically active as well as biologically inactive protein molecules. For Botox to exert its effects, the active proteins must remain intact. However, both types of proteins can be recognized by the immune system as antigens, triggering the production of antibodies. These antibodies bind to the Botox proteins and render them inactive.
If the antibodies bind to molecules that were already biologically inactive, it has no impact on the effectiveness of Botox. However, if the antibodies bind to the biologically active portion of Botox, it blocks its toxic and therapeutic effects.
Recent studies indicate that this blockade can diminish over time. Over a period of 2 to 3 years, the number of antibodies decreases, potentially allowing for successful therapy and the manifestation of Botox’s effects in cases where it previously failed.
Preventing Botox Resistance
The formation of antibodies becomes problematic when Botox is injected in high doses and short intervals. This can be a challenge in neurological therapy, but is unlikely in cosmetic applications.
Administering 50–100 units of Botox every 4–6 months poses a minimal risk for antibody formation. An experienced doctor will take this into consideration and advise against frequent Botox injections in very short intervals (also known as “Botox boosters”). Failure to do so would make the doctor partially accountable for any resulting resistance.
FAQ: Understanding How Botox Works and When to Expect Results
As mentioned earlier, unrealistic expectations contribute to the question of “When does Botox work?” I will now provide a brief FAQ section to explain how Botox works and when its effects become noticeable. This information may help better contextualize the content discussed above.
Botox is a neurotoxin that targets “cholinergic synapses,” which mediate communication between a nerve cell and a downstream cell. This communication occurs through neurotransmitters, with a key neurotransmitter of interest being “acetylcholine.” Botox inhibits the secretion of acetylcholine, thereby interrupting communication between nerve and muscle cells. With this communication disrupted, nerve impulses no longer reach the muscle, resulting in paralysis. This is the basis of Botox’s effectiveness.
After injection, it takes between 24 and 48 hours for the toxin to bind to nerve cells and penetrate them. The process is complex and involves the splitting of the two-part Botox molecule. Only the lighter part, known as the “L-chain,” enters the nerve cell. Inside the nerve cell, Botox cleaves a protein crucial for acetylcholine release, thereby preventing its release.
Consequently, it takes 1–2 days for injected Botox to take effect and for initial muscle paralysis to occur. Some patients notice improvements in their wrinkle appearance from that point onward, but this may not be the case for everyone. Many patients wonder how quickly Botox works and may become anxious after just a few days, especially if it is their first treatment. The time it takes to see the full effects of Botox varies depending on individual factors, particularly the strength and baseline tension of the muscles involved. In my experience, it takes 7–14 days to see the full effects. Men may require slightly longer than women.
Therefore, if you don’t notice any effects after 3, 4, or 5 days, don’t be alarmed. It is normal. However, if after 14 days you still see no results, you should contact your doctor. Usually, a follow-up appointment is already scheduled to address any lack of effect.
In short, no, Botox does not cause long-term effects. The process outlined above for the action of Botox is entirely reversible. The toxin gradually loses its effect until it completely dissipates after 4–6 months. There are no traces or “memory” of Botox left in the body. Therefore, concerns about long-term effects of Botox are unfounded, as confirmed by numerous long-term studies: Botox does not have any long-term effects.
However, muscles can lose strength when they are inactive for a long time. This is a familiar concept for arms and legs. Mimetic muscles are no exception; they also weaken with prolonged immobilization. One could refer to this as a “late-effect of Botox,” but it is only indirectly related to the toxin.

About the author:
Dr. med. univ. Eva Maria Strobl is the owner of LIPS and SKIN Aesthetic Medicine practice in Munich. She is a trained specialist in general medicine (MedUni Vienna) and has over 10 years of specialization in non-surgical aesthetic procedures. She is a member of the German Society for Aesthetic Botulinum Therapy e.V. (DGBT), the German Society of Anti-Aging Medicine e.V. (GSAAM) and of Network Global Health. She publishes regularly on her blog and on DocCheck.
